



Clinical Reasoning for the cervical spine and upper quadrant
by Martin Krause
Elfreda : 27 year old Hairdresser : self employed, sole mother of 2
|
|
What is your Working Hypothesis ?
II: Past history:
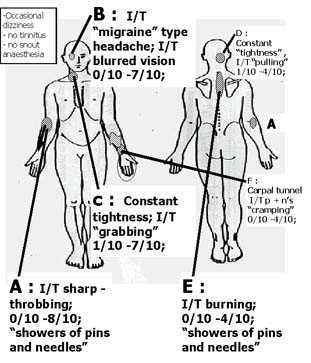
Pain A : nil
Pain B : migraines as a teenager and perhaps 1-2 per year as an adult. Not accompanied by an aura. Usually lasted 24/24 and required occasional medication
Pain C : nil
Pain D : 5 year history of 'muscular tightness' in the back of the neck.
Pain E : 3 year history of 'burning pain' and tightness in the shoulder blade region.
Pain F : 5 year history of 'carpal tunnel' with some p+n's, and 'cramping'.
Hasn't sought treatment for any of these problems in the past. Felt that the majority of problems were stress related due to family problems and business concerns. Also was working in very cold premises until recently.
III: Current History
Pain A began insidiously 18/12 ago as a mild ache. Had been working a little more than usual. Also had a virus at the time. 3/12 ago Pain A increased markedly and changed from an I/T ache to a sharp throbbing pain and more recently into 'showers of pins + needles'. Felt overworked as her employee had been sick.
Pain B began to increase in frequency in the past 6/52.
Pain C began as a 'tightness' approx. 1 year ago. Recently the 'tightness' has been accompanied by 'grabbing' .
Pain D has become a little more intense over the past 6/52.
Pain E increased in intensity and severity 3/12 ago.
Pain F has not changed recently.
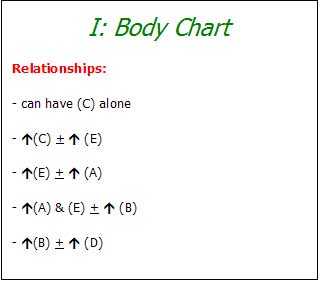
Does the history support the relationship of the pains established on the body chart? Why ?
Is there evidence of abuse, disuse, misuse, overuse?
What is your working hypothesis now?
- structure(s)?
- stage?
- stability?
IV: Aggravating/easing factors
Prolonged cutting and perming (making curls) especially associated with 'colouring' results in increased throbbing pain A 4/10 within an hour. She is right handed.
She can keep working but after 2-3 customers 'showers of pins and needles' may start with pain A reaching 8/10. Generally suffers from cold hands and feet. However, the right arm-hand feels colder when the 'pins & needles' start. Pain E also worsens when Pain A is severe. Usually doesn't take a break but has needed to break for lunch in the past 3 months. However, she doesn't feel that the lunch break rests her sufficiently to reduce the pain completely. Still mild discomfort of pain A 2/10 after 1/24 lunch break.
Pain B appears to worsen with stress. She has noticed that she is holding her right shoulder high and tilting her head to the right whilst cutting. She feels that this position relieves some of the 'tightness' of Pain D & C. However, it may take several hours for the pain in the eye to settle. Furthermore, the blurred vision she finds disturbing. Initially she thought she was getting a stroke.
Pain C worsens with prolonged cutting (~ 2/24). Quick movements result in 'grabbing' like pain 7/10 that settles immediately.
Pain D also appears stress related. Worsens towards the end of the day.
V: 24/24 Behavior
Note
Sleeps well with a contour pillow. However Pain F can wake her at night. Cannot lie on her right elbow. Generally sleeps on her back. Previous to these problems she preferred to sleep on her sides.
morning
Some neck stiffness but generally good.
afternoon
All pains seem to be worse at the end of the day if they have been brought on during the day.
What is the state of the nervous system in terms of possible primary and secondary hyperalgesia?What is the severity and irritability?
What is your working hypothesis in terms of
- structures involved?
- Primary/secondary hypralgesia?
- Neuropathic pain?
- Central pain mechanisms?
What will be the extent of your physical examination?
Is there need for caution? Why?
VI: Physical Examination
|
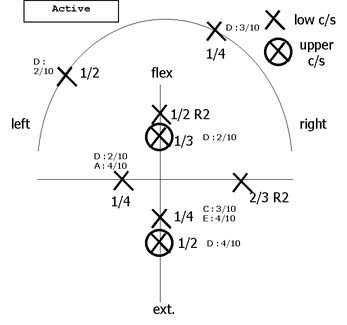
active movement diagram |
Ultt (radial nerve)
Ž 45 abd(A) 6/10 add (L) lat. fl. C/S Ž (A) 8/10, Pain A settled after 5/60 to 1/10 Thoracic outlet test (TOS) Ž (A) 6/10; sl. (B) Slump Ž (E) 3/10; (D)4/10,(C)6/10 with upper C/S extension; Insufficient ROM to test vertebral artery insufficiency |
|
|
|
|
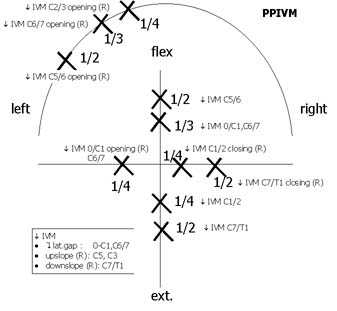
PPIVM
|
Neuro
(right) sensation - slightly reduced over lateral spect of elbow-hand muscle power - decreased finger and thumb extension. |
|
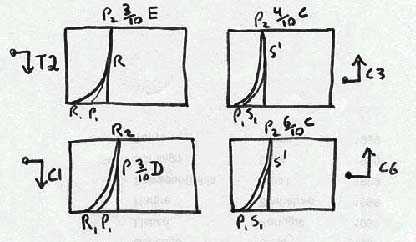
Palpation: decreased Intervertebral Movement (IVM) : C1,C7,T1-5; =C3, C6
|
|
|
|
Did the Physical Examination confirm the
-neuropathic pain? -central pain? What will be your management strategy
How will you measure technique and treatment success?
|
|
 What We do
What We do What We Treat
What We Treat
















































































































